
ALCOHOL AND DRUG USE Michel Tousignant
BIOLOGY AND GENETICS Robert D. Goldney
CULTURE Michel Tousignant
GENDER Silvia Sara Canetto
INDIGENOUS POPULATIONS Ernest Hunter, Desley Harvey
MEDIA EFFECTS Steven Stack
MENTAL ILLNESS Michel Tousignant
PHYSICAL ILLNESS Brian L. Mishara
ROCK MUSIC Laura Proud, Keith Cheng
BIOLOGY AND GENETICS Robert D. Goldney
CULTURE Michel Tousignant
GENDER Silvia Sara Canetto
INDIGENOUS POPULATIONS Ernest Hunter, Desley Harvey
MENTAL ILLNESS Michel Tousignant
PHYSICAL ILLNESS Brian L. Mishara
ROCK MUSIC Laura Proud, Keith Cheng
ALCOHOL AND DRUG USE
Between 30 and 50 percent of persons who die by suicide have a dependence on alcohol or drugs or have shown a pattern of abuse of those substances. The data from four large studies in four different countries confirm this statistic. In a Finnish study led by Markus Henriksson covering all ages over the entire country, diagnoses of dependence and abuse were present in 43 percent of the cases, twice as often in men (39%) as in women (18%). In another study conducted in the United States (San Diego), alcohol abuse was found in 55 percent of cases. Alain Lesage's team in Quebec concluded that 30 percent of male suicide victims below thirty-five had alcohol-dependence problems and that a similar percentage suffered from drug dependence, with a combined dependence rate around 45 percent. Even in South India, where alcohol is difficult to find, Laskmi Rajkumar found in the city of Chennai (formerly Madras) that 35 percent of suicides showed signs of alcoholism.Almost all the alcoholics who commit suicide also suffer from severe mental health problems. In the Finnish study, half of the suicides with alcohol dependence also had a depressive disorder and almost as many had a personality disorder that entailed difficulty in curbing impulsive behavior. In a large 1992 American study research of male alcoholic suicides, directed by George Murphy, researchers found that 72 percent had a depressive disorder and less than a quarter were free of any psychiatric disturbance. The probability that an alcoholic will die by suicide varies from 2 to 6 percent, which is far above that of the American population (1.3%) or the American population without any psychiatric problem (around 1 per 100,000 per year or less than 0.2%).
With respect to illegal drugs, a 1992 study done in New York City found that 15 percent of New York suicides tested positive for cocaine. In Norway Ingebor Rossow found that nearly 3 percent of agroup of patients from both sexes treated for drug dependence had died by suicide after only ten years. Younger people from both sexes have a higher risk, and among them drug abuse leads to suicide more quickly than does alcohol abuse.
Attempted Suicide
Alcohol and drugs also have a major influence on attempted suicides. In a survey sponsored by the National Institute on Alcohol Abuse and Alcoholism in 1992, Deborah Dawson found that those who had frequently become inebriated were more likely to experience suicidal thoughts or to actually try to kill themselves. One out of seven persons who were frequently intoxicated reported suicidal thoughts or attempts compared to 4 percent for other current drinkers. The level rose to 20 percent for those who only used sedatives, tranquilizers, cocaine, or stimulants and to 25 percent in cases of multiple drug use. The link between marijuana and attempted suicide was well documented in a New Zealand study that found that one out of six persons who made serious attempts at suicide were seriously dependent on marijuana.Slow Death and Overdoses
Many people wonder if the use of alcohol and drugs is a way of committing suicide by "slow death." Most persons who abuse these substances are taking them chiefly as a kind of self-medication to reduce their stress. This seems to be more the case with men than with women. A woman who takes to alcohol has often failed to find relief from drugs such as tranquilizers and is more likely to be desperate and vulnerable to suicide. Alcohol also leads to a greater risk of slow death from cirrhosis of the liver and of accidental deaths associated to risk-taking behaviors. Alcohol and drug abuse is also associated with a much higher risk of dying by homicide.The problem of drug overdose is somewhat different. Young homeless adults often attempt suicide by overdosing on illegal drugs. A Norwegian survey by Ingeborg Rossow and Grethe Lauritzen (1999) has shown that nearly half of more than 2,000 drug addicts admitted for treatment reported having experienced at least one life-threatening overdose and that they were six times more likely to have made a suicide attempt than those who had not overdosed. Coroners are still reluctant to classify these deaths as suicides given the difficulty in distinguishing accidents from voluntary gestures.
Alcohol and Drugs As a Cause of Suicide
Do alcohol and drugs directly cause suicide by significantly diminishing the reasoning of the person at the time of the suicide? In the absence of personal data, it is difficult to know if those who drank before committing suicide did so to have the courage to commit suicide. There is evidence, however, to show that alcoholics who commit suicide usually don't act only on the spur of the moment. George Murphy has analyzed the issue of alcohol and impulsivity in a series of ten cases where the person had committed suicide within hours of a very stressful life event. In only two cases was there evidence of an unexpected impulsive act. In six other cases the person had communicated some time before the event his or her intent to die. However, even if the person had considered suicide before, we cannot rule out the possibility of the alcohol triggering an impulsive act. Long-term consumption of alcohol leads to depression, which in turn increases the probability of suicide, according to Murphy's study. But it takes on average more than nineteen years of chronic alcoholism and seven years of depression before reaching this end, which leaves plenty of time for treatment and prevention.If suicide is closely associated with alcohol, is there a direct link between an increase in alcohol consumption and the suicide rate in a population? Despite many attempts to prove this idea, an American study found that the sale of spirits, but not of beer or wine, correlated with increased suicide statistics. The fact that countries that were former members of the Soviet Union have both high rates of suicide and alcoholism supports the hypothesis of a direct link. But we have to wait for more information from China, which has a high incidence of alcoholism and low incidence of suicide, to have a more complete picture. If Islamic countries have both low rates of alcohol and suicides, there are countries such as Mexico or Jamaica where alcohol consumption is high and suicide rates relatively low. One likely explanation is that intoxication in these countries more often take place during religious or social rituals and that these contexts may lessen the adverse consequences of drinking.
The Psychosocial Context
As George Murphy and E. Robins warned physicians in 1967, "The physician should be aware of the critical periods of break in relationships (divorce, separation, mourning) in their alcoholic patients." Later studies comparing cases of alcohol and drug suicide with other suicides have since concluded that the breakup of a love relationship in the six weeks before suicide had more of a causal impact in the alcohol and drug group, perhaps because many alcoholics have suffered rejection and abandonment during childhood and might therefore be more vulnerable to the emotional trauma of separation. Another hypothesis is that the alcoholics progressively enter a process of social isolation, especially during the year before a suicide. Therefore, they may be more vulnerable to a key loss. A Finnish study by Heikkinen found that family discord (38%), financial problems (28%), and marital separations were the chief precipitants of suicides among alcoholics. Persons with an alcohol or drug problems who die by suicide have often alienated friends and family and therefore have little social support.Murphy and his team studied the differences between alcoholics who committed suicide and other alcoholics living in the community. They found that two-thirds of the suicides had had at least four psychosocial risk factors as against only 1 percent in the community alcoholics. Those who committed suicide were twelve times more likely to suffer from a major depression (58% vs. 5%), three times more likely to be unemployed (54% vs. 18%), to live alone (45% vs. 17%), to lack social support (75% vs. 26%), or to have previously made suicide threats (79% vs. 23%). Almost all the suicides were very heavy drinkers (97%), twice as many as in the community alcoholic sample. Twothirds of the suicide cases had four of these risk factors compared with only 1 percent in the community group of alcoholics. Young people with a drug problem who commit suicide are also much more likely to have had a brush with the law, to have a firearm available at home, or to suffer from depression.
Prevention and Intervention
If alcohol and drugs are closely related to suicidal behavior, we cannot conclude that all abusers are at risk. Those who also suffer from depression or a personality disorder are the ones in real danger. Consequently, the treatment of the addiction should also target the other psychological problems. One challenge is to communicate to adolescents that despite the immediate good feelings alcohol or drugs may facilitate, an unpleasant, depressive mood often accompanies abuse. We should recognize that both drugs and alcohol can sometimes alleviate suffering and despair. Limiting alcohol consumption to social rituals may help to minimize the damage in some societies. Furthermore, if alcoholics are working and are supported by their environment, the risk of committing suicide significantly decreases. Both professionals and family members should also realize that alcoholics, especially if middle-aged, are very vulnerable to loss and rejection and that they can benefit from increased social support.The low suicide rate in Islamic countries that limit access to alcohol, contrasted with high rates in the alcohol-consuming West, suggests a direct link between suicide and alcohol abuse. The solution in most countries is not one of repression but rather publicizing the statistical association of suicide with alcohol and drug abuse.
See also: Suicide Influences and Factors: Gender, Mental Illness ; Suicide over the Life Span: Adolescents and Youths, The Elderly ; Suicide Types: Indirect Suicide
Bibliography
Dawson, Deborah A. "Alcohol, Drugs, Fighting and Suicide Attempt/Ideation." Addiction Research 5, no. 6 (1997):451–472.Henriksson, M. M., H. M. Aro, M. J. Marttunen, M. E. Heikkinen, et al. "Mental Disorders and Comorbidity in Suicide." American Journal of Psychiatry 150, no. 6 (1993):935–940.
Lesage, A. D., R. Boyer, F. Grunberg, F. C. Vanier, et al. "Suicide and Mental Disorders: A Case-Control Study of Young Men." American Journal of Psychiatry 151, no. 7(1994):1063–1068.
Marzuk, P. M., K. Tardiff, A. C. Leon, M. Stajic, E. B. Moorgan, and J. J. Mann. "Prevalence of Cocaine Use among Residents of New York City Who Committed Suicide during a One-Year Period." American Journal of Psychiatry 149 (1993):371–375.
Murphy, G. E. Suicide in Alcoholism. New York: Oxford University Press, 1992.
Murphy, G. E., R. D. Wetzel, E. Robins, and L. McEvoy. "Multiple Risk Factors Predict Suicide in Alcoholism." Archives of General Psychiatry 49 (1992):459–463.
Rajkumar, Vijayakumar L. "Are Risk Factors for Suicide Universal? A Case-Control Study in India." Acta Psychiatrica Scandinavica 99 (1999):407–411.
Rossow, Ingebor. "Suicide among Drug Addicts in Norway." Addiction 89 (1994):1667–1673.
Rossow, Ingeborg, and Grethe Lauritzen. "Balancing on the Edge of Death: Suicide Attempts and Life-Threatening Overdoses among Drug Addicts." Addiction 94, no. 2 (1999):209–219.
MICHEL TOUSIGNANT
BIOLOGY AND GENETICS
The possibility that biological and hereditary factors could be related to suicidal behavior has been written about for over 200 years. For example, in 1790 Charles Moore stated that the "propensity to suicide . . . by attacking successive generations of the same family proves itself to be hereditary"; in 1881 in the English translation of his Italian work, Suicide: An Essay on Comparative Moral Statistics, Henry Morselli wrote a chapter entitled "Influences Arising Out of the Biological and Social Condition of the Individual"; and in 1892 the physician Daniel Hack Tuke noted that "examples of hereditary suicides have occurred" (Goldney and Schioldann 2000, pp. 181, 184).There has been considerable debate about the relative importance of biological and hereditary factors as opposed to sociological determinants, and this has led to a split between these two broad explanatory approaches to suicidal behavior. However, twenty-first-century scientists generally recognize that there is a far more subtle interplay between such factors than had previously been understood.
Despite the early descriptive work, it was not until the 1970s that biological and hereditary contributions to suicidal behavior were given a firm scientific basis. In 1976 the Swedish researchers Marie Asberg, Lil Traskman-Bendz, and Peter Thoren demonstrated a lowered level of five hydroxy indole acetic acid (5-HIAA) in the cerebrospinal fluid (CSF) of suicide attempters who had used violent methods, and suggested that it may be a biochemical suicide predictor. This was important as CSF 5-HIAA is a breakdown product of serotonin, one of the neurotransmitters associated with mood and behavior disturbances. In 2000 Traskman-Bendz and John Mann reviewed subsequent studies from a number of different centers, and found that there is general agreement within scholarship that those people with low CSF 5-HIAA have a higher likelihood of committing suicide. They also noted that other primate studies have shown a relationship between low CSF 5-HIAA and aggression.
The importance of serotonin transmission has also been demonstrated by postmortem studies, where in 1995 Victoria Arango, Mark Underwood, and John Mann reported reduced binding to serotonin transporter sites in the ventral prefrontal cortex of the brain of completed suicides compared to those who died from other causes.
The activity of another neurotransmitter, dopamine, has also been examined by measuring the growth hormone response to apomorphine in depressed persons, some of whom later suicided. In 2001 William Pitchot and his Belgian colleagues reported a significantly lower response in eight male depressed patients who suicided compared to eighteen depressed patients who had never attempted suicide, leading them to conclude that dopamine was involved in the biology of suicide in depression.
Further evidence of the importance of neurotransmitters and the hypothalamic-pituitary-adrenal axis has emerged from a fifteen-year follow-up study of depressed patients who had had the dexamethasone suppression test during their initial assessment. In a 2001 study conducted at the University of Iowa, William Coryell and Michael Schlesser reported that 7 of the 8 suicides out of 78 patients had been nonsuppressors of cortisol, a biological indicator of their depressive condition. They reported that nonsuppression increased the likelihood of future suicide fourteenfold.
The role of corticotropin-releasing factor (CRF) has also been examined in completed suicides. Researchers have reported a reduction of CRF binding sites in the frontal cortex of the brain. Although not all studies concur with this finding, the role of CRF may still be important, as studies reviewed in 1999 by Christine Heim and Charles Nemeroff have demonstrated that early life stress produces persistent elevated CRF activity, which is associated with increased reactivity to stress in adult life. They suggest that stress at critical stages of development in people with a genetic predisposition could result in neurobiologically vulnerable adults who were more likely to develop mental disorders following exposure to further stress.
The hereditary basis to suicide was first convincingly described by Fini Schulsinger and his colleagues in 1979 in a Danish adoption study, which examined individuals who were separated at birth from their biological relatives. Using a matched control design, more of the biological relatives of the adopted suicides committed suicide compared to the biological relatives of adopted controls. Subsequent research has suggested that the genetic factor could be related to impulse control independent of mental disorder. Since Schulsinger's early study, there have been important developments in genetic studies that have been reviewed by others. For example, in 2000 Alec Roy and colleagues reported that in 399 suicide twin pairs in the literature, there was 13.2 percent concordance for suicide in the 129 identical (monozygous) twins, compared to 0.7 percent concordance for suicide in the 270 non-identical (dizygous) twin pairs.
The extent of the possible contribution of genetic factors to suicidal behavior has been illustrated well in a 1998 study of 5,995 Australian twins. In a sophisticated logistic regression analysis, which allowed for sociodemographic, personality, psychiatric, traumatic event, and family history variables, no less than 45 percent of the variance in suicidal thoughts and behavior was related to genetic factors. Furthermore, after controlling for those variables, a history of suicide attempt or persistent suicidal thoughts in a co-twin remained a significant predictor of suicidal thoughts and behavior in identical twins, but not in nonidentical twin pairs.
Other genetic studies have focused on possible associations between suicidal behavior and genetic variance in the serotonin system. In particular, the enzyme tryptophan hydroxylase (TPH), which is the rate-limiting enzyme in the synthesis of serotonin, has been examined in detail. In a 2001 review and further study, Gustavo Turecki and colleagues noted that most research has been carried out on those who had attempted suicide. They investigated 101 suicide completers and could not replicate previous research, although they found another genetic variation to be more frequent in suicides than in normal controls. They referred to "the substantial role that the gene that codes for TPH may play in the neurobiology of suicidal behavior," but it is not clear whether it is related to psychiatric disorders or to personality traits such as impulsivity (Turecki 2001, p. 98 ).
Biological and hereditary factors do not operate independently, and do not inevitably lead to suicide in any individual, even if there is a strong family history of suicide. Rather, they can only increase the susceptibility of some individuals to react more severely to stress. The relationship between stress and neurobiological reactions has been reviewed from an ethological perspective, and there are persuasive primate as well as human studies that have added weight to the theory of Robert Post in 1992 about the role of stress in producing depression, the psychiatric condition most frequently associated with suicide.
The finding of significant biological and genetic determinants of suicidal behavior does not negate the importance of the individual and his or her psychosocial environment. Therefore the results of any of the individual studies referred to need to be considered with caution, and integrated into science's existing psychosocial understanding of suicidal behavior.
See also: Suicide ; Suicide Influences and Factors: Gender, Mental Illness
Asberg, Marie, Lil Traskman, and Peter Thoren. "5-HIAA in the Cerebrospinal Fluid: A Biochemical Suicide Predictor?" Archives of General Psychiatry 33 (1976):1193–1197.
Coryell, William, and Michael Schlesser. "The Dexamethasone Suppression Test and Suicide Prediction." American Journal of Psychiatry 158 (2001):748–753.
Goldney, Robert D. "Ethology and the Suicidal Process." In Kees van Heeringen ed., Understanding Suicidal Behaviour. Chichester, England: John Wiley and Sons, 2001.
Goldney, Robert, and Johann Schioldann. "Pre-Durkheim Suicidology." Crisis 21 (2000):181–186.
Heim, Christine, and Charles B. Nemeroff. "The Impact of Early Adverse Experiences on Brain Systems Involved in the Pathophysiology of Anxiety and Affective Disorders." Biological Psychiatry 46 (1999):1509–1522.
Hucks, David, et al. "Corticotropin-Releasing Factor Binding Sites in Cortex of Depressed Suicides." Psychopharmacology 134 (1997):174–178.
Kety, Seymour. "Genetic Factors in Suicide." In Alec Roy ed., Suicide. Baltimore, MD: Williams and Wilkins, 1986.
Nemeroff, Charles B., et al. "Reduced Corticotropin-Releasing Factor Binding Sites in the Frontal Cortex of Suicide Victims." Archives of General Psychiatry 45 (1988):577–579.
Pitchot, William, et al. "Reduced Dopaminergic Activity in Depressed Suicides." Psychoneuroendocrinology 26 (2001):331–335.
Post, Robert M. "Transduction of Psychosocial Stress into the Neurobiology of Recurrent Affective Disorder." American Journal of Psychiatry 149 (1992):999–1010.
Roy, Alec, et al. "The Genetics of Suicidal Behavior." In Keith Hawton and Kees van Heeringen eds., The International Handbook of Suicide and Attempted Suicide. London: John Wiley and Sons, 2000.
Schulsinger, Fini, et al. "A Family Study of Suicide." In Mogens Schou and Erik Stromgren eds., Origin, Prevention and Treatment of Affective Disorders. New York: Academic Press, 1979.
Statham, Dixie J., et al. "Suicidal Behavior: An Epidemiological and Genetic Study." Psychological Medicine 28 (1998):839–855.
Traskman-Bendz, Lil, and John J. Mann. "Biological Aspects of Suicidal Behavior." In Keith Hawton and Kees van Heeringen eds., The International Handbook of Suicide and Attempted Suicide. London: John Wiley and Sons, 2000.
Turecki, Gustavo, et al. "TPH and Suicidal Behavior: A Study in Suicide Completers." Molecular Psychiatry 6 (2001):98–102.
Bibliography
Arango, Victoria, Mark D. Underwood, and J. John Mann. "Postmortem Findings in Suicide Victims: Implications for In Vivo Imaging Studies." Annals of the New York Academy of Sciences 836 (1997):269–287.Asberg, Marie, Lil Traskman, and Peter Thoren. "5-HIAA in the Cerebrospinal Fluid: A Biochemical Suicide Predictor?" Archives of General Psychiatry 33 (1976):1193–1197.
Coryell, William, and Michael Schlesser. "The Dexamethasone Suppression Test and Suicide Prediction." American Journal of Psychiatry 158 (2001):748–753.
Goldney, Robert D. "Ethology and the Suicidal Process." In Kees van Heeringen ed., Understanding Suicidal Behaviour. Chichester, England: John Wiley and Sons, 2001.
Goldney, Robert, and Johann Schioldann. "Pre-Durkheim Suicidology." Crisis 21 (2000):181–186.
Heim, Christine, and Charles B. Nemeroff. "The Impact of Early Adverse Experiences on Brain Systems Involved in the Pathophysiology of Anxiety and Affective Disorders." Biological Psychiatry 46 (1999):1509–1522.
Hucks, David, et al. "Corticotropin-Releasing Factor Binding Sites in Cortex of Depressed Suicides." Psychopharmacology 134 (1997):174–178.
Kety, Seymour. "Genetic Factors in Suicide." In Alec Roy ed., Suicide. Baltimore, MD: Williams and Wilkins, 1986.
Nemeroff, Charles B., et al. "Reduced Corticotropin-Releasing Factor Binding Sites in the Frontal Cortex of Suicide Victims." Archives of General Psychiatry 45 (1988):577–579.
Pitchot, William, et al. "Reduced Dopaminergic Activity in Depressed Suicides." Psychoneuroendocrinology 26 (2001):331–335.
Post, Robert M. "Transduction of Psychosocial Stress into the Neurobiology of Recurrent Affective Disorder." American Journal of Psychiatry 149 (1992):999–1010.
Roy, Alec, et al. "The Genetics of Suicidal Behavior." In Keith Hawton and Kees van Heeringen eds., The International Handbook of Suicide and Attempted Suicide. London: John Wiley and Sons, 2000.
Schulsinger, Fini, et al. "A Family Study of Suicide." In Mogens Schou and Erik Stromgren eds., Origin, Prevention and Treatment of Affective Disorders. New York: Academic Press, 1979.
Statham, Dixie J., et al. "Suicidal Behavior: An Epidemiological and Genetic Study." Psychological Medicine 28 (1998):839–855.
Traskman-Bendz, Lil, and John J. Mann. "Biological Aspects of Suicidal Behavior." In Keith Hawton and Kees van Heeringen eds., The International Handbook of Suicide and Attempted Suicide. London: John Wiley and Sons, 2000.
Turecki, Gustavo, et al. "TPH and Suicidal Behavior: A Study in Suicide Completers." Molecular Psychiatry 6 (2001):98–102.
ROBERT D. GOLDNEY
CULTURE
Anthropology, comparative psychiatry, and psychology have contributed with their specific approaches to better analyze the cultural processes leading to suicide. This rich literature presents new ways of understanding the causes and the influences of suicide on the models of explanation and on specific ways of prevention.Universality of Suicide
Suicide has been known to humanity since the beginning of time and can be found in the mythologies and legends of the great civilizations. There was a Mayan goddess named Ixtab who protected those who had died by suicide. In Virgil's Aeneid, Dido, queen of Carthage, took her life after Aeneas reluctantly left her to continue his mission. Several suicides are depicted in the Bible, but most characters profiled were trying to avoid a life-threatening and shameful situation like falling prey to the enemy.Suicide was present in many cultures before any contact with the conquering Europeans. The Maoris of New Zealand were known to have had a high tolerance toward suicide. There was a famed cliff where people would jump and the port of Whangaroa presumably took its name from a word meaning suicide. The scholar Fredrick Maning believed that as early as 1843 suicide occurred every day among this people. A famous legend told of TeAohuruhuru, a young bride of great beauty, who had been dishonored by her husband when he unveiled her naked body to friends while she was sleeping. As revenge, she drowned herself in front of his boat.
In a 1985 overview of the Bimin-Kuskusmin and other groups of New Guinea, the anthropologist Fitz Poole found that their contemporary high rates of suicide had preceded acculturation and suicides were present during a period when inter-tribal warfare and cannibalism were not yet eradicated. Poole estimated that as much as 10 percent of deaths over the last six generations were by suicide. During a trip around 1970 he counted thirty suicides, which accounted for 57 percent of all deaths. The men who committed suicide were mostly in their early twenties and were trying to avoid making war; the women were stressed by the high number of male victims and by being forced to participate in cannibalism.
Cross-Cultural Picture of Suicide
Many countries report their suicidal rates to the World Health Organization (WHO). These rates are difficult to compare because the methods of recording vary between countries and even within geographical areas of a single country. For instance, the Indian sociologist Soltamin Aleem reported in 1994 that the rate was near 25 per 100,000 annually in the state of Kerala, a state of Southwestern India with a relatively high level of education and distribution of income, and below 1 per 100,000 in the state of Bihar, which is paradoxically one of the poorest states of India. For this reason, the anthropologist Robert Desjarlais concluded that the variations between nations were dependent upon the ability of local institutions to complete valid investigations. He quoted two field studies in North India that yielded rates three to five times the national rates.The most recent rates reported to WHO in the year 2001 show that the highest ranking countries, with a rate above 16 suicides per 100,000 individuals per year, cover a large area, including the Baltic states, some countries of the former Eastern Europe, the federation of Russia, China, Japan, and Sri Lanka. In Western Europe, the rates are in the same range for Austria, France, and Switzerland. The rest of Western Europe, as well as the United States and Canada, was in the category of between 8 and 16 suicides per 100,000 per year, which also includes Australia and India. The countries from Latin America are in the lower range, with the exception of Cuba. The majority of the governments from the African continent did not report any data.
Rates of suicide also tend to vary little when members from a culture migrate to another country, as was found in Australia and the United States, at least during the first years of settlement, and they tend toward the rate of the host country as the years progress. The rates of suicide also vary within the ethnic groups of one country. For example, the rate for the large Hungarian community in Romania is more similar to that of Hungary than to that of the rest of Romania. The African-American population of the United States has a slightly lower rate than the national rate despite the group's lower average income. In the southwestern states, the rate is half for Latinos as compared to Anglos. However, a 1999 study on youth by the Centers for Disease Control showed that Latinos were more likely than African Americans or European Americans to have seriously considered attempting suicide. Consequently, the portrait of suicide and culture in the United States may change significantly in the upcoming decades of the twenty-first century.
Tworeports from 1960 show that suicide was far from unknown in sub-Saharan Africa even before the end of colonization. Local reports from Uganda, Zambia, and South Africa illustrate a significant presence of suicide there, with a rate around 10 per 100,000. For example, the anthropologist Ellen Brown reported twelve cases among the Sara Nar of Chad, which corresponds to a rate of 20 per 100,000.
Suicide and the Mental Health of a Society
The rate of suicide is one of the many factors that reflect the mental health of a population. Suicide often indicates how a certain range of people with psychiatric or adaptation problems are excluded from social or family life rather than providing a good estimate of the happiness of a population. The rates of depression, alcoholism, or suicide attempts are more reliable indices of the mental state of a population. However, a suicide rate cannot be a good argument against a sociopolitical system. During his presidency, Dwight D. Eisenhower had been critical of the social democratic system in Sweden on the grounds that Sweden had a high suicide rate when, in fact, the Swedish rate had reached a peak during the country's period of capitalism.Conceptions of Suicide across Cultures
The cultural attitudes of tolerance toward or repression against suicide probably influence individual choices about committing suicide. Sometimes a religion condones certain forms of sanctified suicides while condemning this mode of exit from life for the common people. The Hindu religion is a good example. In 1998 the anthropologist Karin Andriolo described how the Hindu society considered taking one's own life as a welcomed departure when a person had reached a state of perfection. In "The History of Suicide in India," Upendra Thakur documented many characters of high and low origin who committed suicide in narration of the religious texts. However, during the period of Dharmasastras, one of the sacred books, suicide was determined to be a sin and the suicide victim deprived from death rituals. In the modern period, suicide is viewed as shameful for the family.In Bangalore, India, women are often accused of being the cause of suicide as shown in a 1998 survey conducted by Michel Tousignant, Shekhar Seshadri, and Anthony Raj. If women commit suicide, they are said to be ashamed of having transgressed a rule; if men commit suicide, they are thought to have been the victim of some form of abuse at the hands of a woman. This article also mentions that sati, the suicide by the self-immolation of a widow on her husband's pyre, is still romanticized by a wide section of the Indian population. There is a ban on sati and it has been determined that some modern cases of sati were not suicides but rather disguised homicides.
In Haiti public perception is that suicide is extremely rare. In this society, suicide is unacceptable among the poor because it is considered an example of letting down friends in their fight against the adversities of life. On the other hand, in 1998 the anthropologist Jeanne Marecek, working in Sri Lanka, found little tolerance of suicide despite the high rate in this country. The population attributes this gesture to the conditions of life, such as unemployment or romantic problems, and people are usually ready to give support to persons who have made an attempt.
In sub-Saharan countries many traditional religions view suicide as impure. In Uganda people avoid coming into contact with the corpse of a person deceased by suicide and in Rwanda survivors burn the person's possessions. A Senegal oral tradition requires that someone who comes across a person who died by suicide should make a sacrifice, and in Nigeria the body is buried on the spot, without any ritual.
Theories
The French sociologist Émile Durkheim's theory about suicide, which came into prominence at the end of the nineteenth century, was cultural. His argument claimed that regions with the highest rates of suicide were in a relative state of anomie; that is, situations where the rules guiding a society were either absent or weak. Similarly, societies with a relative absence of social integration were considered hardest hit by suicide. One of his points was that Jews and Catholics had low rates because they formed more cohesive groups, while Protestants had high rates because their relationship to God was more personal. This theory is still useful in understanding how rates are becoming higher in rapidly acculturating groups such as the Aboriginal peoples of Northern Canada, Greenland, Brazil, and the Melanesian islands. The rapid change from a nomadic to a sedentary life, the spread of alcoholism, the lack of access to modes of production, the changing patterns of family structure, abuse and incest, and racial discrimination from the dominant society are often the elements of the cultural breakdown.However, the fact that people committing suicide are mostly young males calls for a less global explanation. The sociologist Francis Hezel has shown that suicide, as well as alcoholism in Melanesia, is a way of escaping social contradictions by young people with little faith in their future. The younger generation is often schooled to foreign values, far away from their families, and is later scorned by parents who have lost their moral authority over them. Not being able to adopt any model, these young people choose not to participate in life by committing suicide.
In China and in India where the rate of female suicide is very similar to that of males (in contrast to the ratio of one to four in many countries), women move to their in-laws' homes after marriage. One likely explanation of female suicides is that when repeated conflicts take place, not only is it shameful and in some cases impossible for the women to return to their families, they are threatened to be deprived of contact with their children.
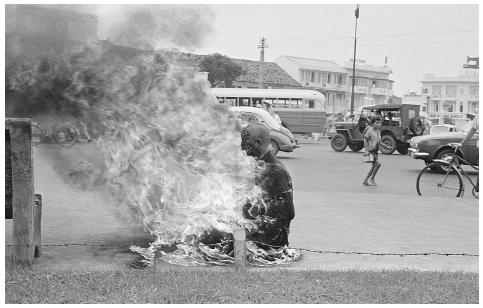
In a form of ritual suicide, Buddhist monks in Saigon who protested the violence demonstrated by the Ngo Dinh Diem government during the Vietnam war died by self-immoliation in an open public square.
BETTMANN/CORBIS
In Western countries, men often commit suicide after the end of their marriage, sometimes after a long period of alcoholism when they have alienated their friends and relatives by their conduct. Here, they are the ones who are estranged from their children and who find themselves in a state of solitude and low social support.
Scholars confess the theoretical challenge in explaining why suicide is nearly absent in certain societies. In North Africa as well as in sub-Saharan Africa, many authors have identified the low prevalence of guilt and the habit of projecting aggression onto others rather than criticizing oneself, as well as the tendencies to express stress in bodily symptoms rather than by emotional means. These modes of expressing stress may eventually protect against depression and suicide.
The 2000 review of the sociologist Steven Stack on religion and suicide has contributed to a different perspective on some of Durkheim's ideas. First, there is mixed support in the United States for the hypothesis that Catholics are more protected from suicide than people from other religions and no support for this statistic is found in Canada. Reanalysis of data from 1905 to 1910 in the Netherlands suggests that Catholics may have been hiding some of their cases of suicide. However, a survey of seventy nations has shown that a high rate of Islamics in the country was associated with a lower suicide rate. There is some evidence that religious commitment may be a protective factor despite the fact that many studies have refuted this hypothesis. The connection between religion and suicide is weak and most studies indicate little about the religious status of those who have committed suicide, making it difficult to analyze the connection.
Prevention and Intervention
One of the most promising interventions has come from Sri Lanka in a project asking volunteers to travel to villages where suicide is spreading and to support families in which a member has died from suicide. In the United States, the Centers for Disease Control issued guidelines for Aboriginal communities that can be used with similar groups. Scholars maintain that prevention should be done both at the community level, to promote the sense of pride and efficacy of the group, and at the individual level, to follow up with those who are recognized as threatened, such as in schools and in emergency services. Because social scientists often find a situation of social rejection within certain ethnic groups, or the marginalization of certain persons within these groups, efforts to valorize these cultures is a first step toward preventing suicide.In 1999 the researchers Michael Phillips, Huaqing Liu, and Yanping Zhang reported that there are more than 300,000 suicides a year in China. There is little recognition of depression and it is estimated than only 5 percent of the cases of clinical depression are currently treated. They proclaim that a wider access to treatment of depression and support would help prevent suicide. Since the rate is higher in rural areas where emergency medicine is not readily available, the researchers maintain that there should be a better control of pesticides, which is one of the most readily available and lethal ways of dying by suicide in that country.
Approximately 1 million people die from suicide each year around the world. Suicide is becoming an international public health concern on the same level as illnesses such as malaria. Researchers are in a position to verify that the experience of some cultures is being repeated elsewhere. For example, the suicide contagion experienced among rapidly acculturating Aboriginal peoples has started to appear in Brazil. Because of this prevalence, there is an urgency among social scientists to address suicide as soon as it appears among certain people groups, and to rapidly apply learned lessons in order to suggest methods of prevention.
See also: Durkheim, É MILE ; Suicide ; Suicide Basics: History ; Suicide Influences and Factors: Indigenous Populations
Bibliography
Andriolo, Karin R. "Gender and the Cultural Construction of Good and Bad Suicides." Suicide and Life-Threatening Behavior 28 (1998):37–49.Desjarlais, Robert, Leon Eisenberg, Byron Good, and Arthur Kleinman. World Mental Health: Problems and Priorities in Low-Income Countries. New York: Oxford University Press, 1995.
Hezel, Francis X. "The Cultural Patterns in Trukese Suicide." Ethnology 23 (1984):193–206.
Marecek, Jeanne. "Culture, Gender, and Suicidal Behavior in Sri Lanka." Suicide and Life-Threatening Behavior 28 (1998):62–68.
Phillips, Michael R., Huaquing Liu, and Yanping Zhang. "Suicide and Social Change in China." Medicine and Psychiatry 23 (1999):25–50.
Poole, Fitz. "Among the Boughs of the Hanging Tree: Male Suicide among the Bimin-Kuskusmin of Papua New Guinea." In Francis Hezel, Donald Rubenstein, and Geoffrey White eds., Culture, Youth and Suicide in the Pacific: Papers from the East-West Center Conference. Honolulu: East-West Center, 1985.
Stack, Steven. "Suicide: A 15-Year Review of the Sociological Literature: Part II Modernization and Social Integration Perspectives." Suicide and Life-Threatening Behavior 30 (2000):163–176.
Thakur, Upendra. The History of Suicide in India. Delhi: Munshi Ram Manohar Lal, 1963.
Tousignant, Michel, Shekhar Seshadri, and Anthony Raj. "Gender and Suicide in India: A Multiperspective Approach." Suicide and Life-Threatening Behavior 28 (1998):50–61.
MICHEL TOUSIGNANT
GENDER
Consistent with current scholarship, gender, like race, is conceptualized as a social construct rather than as an attribute of individuals. It is what cultures make of the fact that a person is a woman or a man. Gender is also what cultures define as appropriate behavior for women and men across a variety of situations, including situations of distress. Finally, gender, like race, is a status variable determining a person's location in the social hierarchy, including the barriers and resources that a person will likely encounter.Patterns of Suicidal Behavior by Culture
In the United States women and men tend to engage in different kinds of suicidal behavior. Women are more likely to engage in nonfatal suicidal behavior, while men are more likely to die as a result of a suicidal act. In 1998 the researchers Silvia Sara Canetto and Isaac Sakinofsky called this phenomenon the gender paradox of suicidal behavior. United States gender patterns of suicidal behavior are similar to those found in other English-speaking countries, such as Canada and Australia. They are different, however, from those observed in a variety of other countries. For example, in Finland and in India, men have similar rates of nonfatal suicidal behavior as women. Furthermore, in China, it is women who typically die of suicide. China accounts for 21 percent of the world's population, 44 percent of the world's suicides, and 56 percent of the world's female suicides. Exceptions to the male predominance among those who die of suicides are also found within some ethnic communities in the United States. For example, according to a 1997 San Francisco study by Julia Shiang and colleagues, Asian-American women aged eighty-five and older have twice the rates of suicide mortality of same-aged Asian-American men.Suicide methods are culturally specific. Common suicide methods in one culture may be unusual in another. Women and men tend to use the methods that are culturally permissible for them in their culture, not just those that are accessible. In some cultures, women and men use different suicide methods; in other cultures they use the same methods. Since the 1990s firearms have been the most common method of suicide in the United States with both women and men. However, they account for a greater proportion of men's than women's suicides (two-thirds vs. one-third). By contrast, in Canada women still prefer poisoning as a method of suicide, and men firearms. However, Canadian men's preference for firearms as a method of suicide is lower than that of U.S. women. In addition, among the Inuit of Canada, an Aboriginal hunting community, the most common method of suicide is hanging, despite the widespread availability of firearms.
Adolescent Suicidal Behavior in the United States
Gender patterns of suicidal behavior vary by age across the life span. In the United States adolescent girls are two to three times more likely to report being suicidal than adolescent boys. Suicidal ideation appears to be particularly common among Mexican-American youth. Adolescent girls are also more likely than adolescent boys to engage in nonfatal acts of suicidal behavior by an average ratio of three to one. Approximately one in ten adolescent girls reports having engaged in suicidal behavior. Gender differences in nonfatal suicidal behavior are not found in all ethnic groups in the United States. For example, among native Hawaiians and Native Americans, adolescent girls report similar rates of nonfatal suicidal behavior as adolescent boys. Rates of nonfatal suicidal behavior appear to be particularly high among Mexican-American girls. Nonfatal suicidal behavior is more common among adolescents from lower socioeconomic classes such as adolescents whose parents are not as well educated. Homosexual adolescent males have high rates of nonfatal suicidal behavior, relative to heterosexual males. Rates of nonfatal suicidal behavior decline after adolescence in women and men.Suicide rates in U.S. adolescent males exceed those of their female peers by a ratio of five to one. The gender difference in mortality holds across ethnicity, although suicide rates vary greatly from group to group. Native-American boys have higher rates of suicide than Native-American girls, although the latter have higher rates of suicide than European-American boys. No definitive information is available on rates of death by suicide among homosexual males.
Adult Suicidal Behavior in the United States
For women, suicide rates remain low throughout the life span, with a small peak around forty-five years of age. For men, on the other hand, rates of suicide increase after sixty years of age. This is particularly true among males of European-American backgrounds. The female-to-male suicide ratio for those aged sixty-five and above hovers around one to six. There are ethnic variations in gender patterns of suicide mortality across the life span. For example, rates of suicide for Chinese-American women rise after the age of forty-five, and reach a peak in late adulthood.Explanations for Gender Patterns of Suicidal Behavior
Most theories of gender and suicidal behavior have overlooked the local and international cultural variability in patterns of gender and suicidal behavior. Overgeneralizing from U.S. national trends, theorists have asked questions like, Why do women engage in more suicidal behavior and why do men die of suicide, instead of questions like, Why are women in some cultures more likely than men to engage in suicidal behavior? or Why are men in some cultures more likely to kill themselves than women? As a result, most theories fail to account for the variations in gender patterns of suicidal behavior found both within and beyond the United States. For example, it has been argued that suicide in older adults is a response to the losses of aging (e.g., reduced financial resources, widowhood, and poor health). This theory does not take into account that in some cultures rates of suicide are low in both older women and older men. It also fails to explain why in many countries, including the United States, suicide is rare in older women, despite the fact that that older women experience more social, economic, and health problems than older men.The theory of cultural scripts, which is based on the observation of a correspondence between cultural norms and behavior, addresses cultural variations in gender and suicidal behavior. According to this theory, individuals tend to engage in the behaviors (including suicidal behaviors) that are meaningful and permissible for people like them in their culture. Each culture has its own models and rules for suicidal behavior. There are specific conditions under which suicidal behavior is expected, and by whom. In other words, there are different scripts of suicidal behavior. These scripts define the scenario of the suicidal act (including the actor, the method, the precipitants, and the themes) as well as the consequences of the suicidal behavior. When suicidal behavior becomes a possibility, these scripts, transformed and individualized, provide a blueprint for action.
What are the cultural scripts of gender and suicidal behavior in the United States? Studies indicate that it is considered unmasculine to admit to suicidal thoughts. Nonfatal suicidal behavior is considered less masculine and less potent than fatal suicidal behavior. "Feminine" persons are expected to "attempt" suicide more than "masculine" persons. Males are particularly critical of other males who survive a suicidal act. Studies also show that killing oneself is seen as a masculine and relatively strong act: Male suicide is not judged as less wrong or less foolish than female suicide. Men who kill themselves are viewed as better adjusted than women who kill themselves, independent of the reasons for the suicide. Men are also more likely to agree with and accept a suicidal decision than women. These meanings and attitudes have been particularly well documented among adolescents and young adults.
Given these gendered messages about suicidal behavior, some scholars are not surprised by the fact that in the United States females are more likely to engage in nonfatal suicidal behavior but are less likely than males to kill themselves. The association of femininity and nonfatal suicidal behavior may be a factor in women's high rates of nonfatal suicidal behavior. At the same time, the association of suicide with masculinity may protect females against killing themselves. Research has also shown that identification with behaviors considered feminine, independent of sex, is associated with increased risk for nonfatal suicidal behavior. For example, homosexual and bisexual males who score high on a measure of conventional femininity are more likely to have a history of nonfatal suicidal behavior.
Prevention
The data on cultural scripts of gender and suicidal behavior suggest new directions for the prevention of suicidal behavior both in educational programs as well as in interventions with suicidal persons. Social scientists and health care professionals believe prevention programs and clinical interventions should educate about the epidemiology of gender and suicidal behavior across sexual orientation, social class, and culture. These prevention programs should assess beliefs about gender and suicidal behavior. Furthermore, they should challenge potential dysfunctional beliefs, such as the idea that nonfatal suicidal behavior is an acceptable way for young women to cope with problems, or the idea that killing oneself is powerful and masculine.In terms of prevention, a promising finding is that androgynous persons tend to view the decision to kill oneself as foolish, independent of the reason for the suicidal wish. They also report less agreement, acceptance, and sympathy for such a decision. Researchers believe it may be that androgyny is associated with greater cognitive and behavioral resourcefulness and flexibility. This is not surprising given that androgynous persons are high in conventionally feminine traits, such as expressiveness, as well as in conventionally masculine traits like instrumentality. These findings suggest that suicide prevention programs may be more effective if they address the limitations that gender ideologies impose on coping, and if they encourage the development of androgynous behavior.
See also: Grief: Gender ; Suicide ; Suicide Basics: Epidemiology ; Suicide Influences and Factors: Gender
Bibliography
Canetto, Silvia Sara. "Gender and Suicidal Behavior: Theories and Evidence." In Ronald W. Maris, Morton M. Silverman, and Silvia Sara Canetto eds., Review of Suicidology. New York: Guilford, 1997.Canetto, Silvia Sara. "Meanings of Gender and Suicidal Behavior among Adolescents." Suicide and Life-Threatening Behavior 27 (1997):339–351.
Canetto, Silvia Sara, and David Lester. "Gender, Culture and Suicidal Behavior." Transcultural Psychiatry 35 (1998):163–191.
Canetto, Silvia Sara, and David Lester. "Gender and the Primary Prevention of Suicide Mortality." Suicide and Life-Threatening Behavior 25 (1995):58–69.
Canetto, Silvia Sara, and David Lester. Women and Suicidal Behavior. New York: Springer, 1995.
Canetto, Silvia Sara, and Isaac Sakinofsky. "The Gender Paradox in Suicide." Suicide and Life-Threatening Behavior 28 (1998):1–23.
Dahlen, Eric R., and Silvia Sara Canetto. "The Role of Gender and Suicide Precipitant in Attitudes toward Nonfatal Suicidal Behavior." Death Studies 26 (2001): 99–116.
Kral, Michael. "Suicide and the Internalization of Culture: Three Questions." Transcultural Psychiatry 35 (1998):221–233.
Lester, David. "Suicide among the Elderly in the World: Covariation with Psychological and Socioeconomic Factors." In Diego De Leo ed., Suicide and Euthanasia in Older Adults. Seattle, WA: Hogrefe & Huber, 2001.
Murray, Christopher J. L., and Alan D. Lopez. The Global Burden of Disease. Cambridge, MA: Harvard University Press, 1996.
Pritchard, Colin. "Suicide in the People's Republic of China Categorized by Age and Gender: Evidence of the Influence of Culture on Suicide." Acta Psychiatrica Scandinavica 93 (1996):362–367.
Remafedi, Gary. "Suicide and Sexual Orientation." Archives of General Psychiatry 56 (1999):885–886.
Shiang, Julia, Robert Blinn, Bruce Bongar, Boyd Stephens, Donna Allison, and Alan Schatzberg. "Suicide in San Francisco, CA: A Comparison of Caucasian and Asian Groups, 1987–1994." Suicide and Life-Threatening Behavior 27 (1997):80–91.
Yee, Darlene. "Issues and Trends Affecting Asian Americans, Women and Aging." In Jean M. Coyle ed., Handbook on Women and Aging. Westport, CT: Greenwood Press, 1997.
SILVIA SARA CANETTO
INDIGENOUS POPULATIONS
In the mid-1990s, during the course of a national commission into indigenous affairs, the Royal Commission on Aboriginal Peoples released a special report on Aboriginal suicide, stating:Collective despair, or collective lack of hope, will lead us to collective suicide. This type of suicide can take many forms, foreshadowed by many possible signs: identity crisis, loss of pride, every kind of dependence, denial of our customs and traditions, degradation of our environment, weakening of our language, abandonment of our struggle for our Aboriginal rights, our autonomy and our culture, uncaring acceptance of violence, passive acknowledgment of lack of work and unemployment, corruption of our morals, tolerance of drugs and idleness, parental surrendering of responsibilities, lack of respect for elders, envy of those who try to keep their heads up and who might succeed, and so on. (Royal Commission on Aboriginal Peoples 1995, p. 38)Chief Jean-Charles Piétacho of the Mingan First Nation, whose submission is included in a special report from 1995 on Aboriginal suicide for the Canadian Royal Commission on Aboriginal Peoples, might have been speaking of indigenous suicide in any of the nations with histories of Anglo-settler colonialism. The indigenous peoples of Canada, the United States, Australia, and New Zealand were all exposed to colonization, dispossession, and depopulation through disease and violence. This was, arguably, most recent and devastating for Aboriginal Australians. Among the outcomes of these histories are levels of disease and ill health that are worse than for nonindigenous nationals. Using the crude proxy of the gap in life expectancy between indigenous and non-indigenous peoples in each nation, health inequality is also greatest for Aboriginal Australians, being shorter by nearly two decades. In all four countries, indigenous suicide has been recognized and systematically addressed as a major health issue in Australia only since the 1990s. Finally, indigenous suicide in all four countries occurs against a backdrop of increasing national rates of suicide for young men. For each of these countries, overall suicide rates for men between the ages of fifteen and twenty-four are high in comparison with most other industrialized nations, ranging between 20 and 40 per 100,000 in the early 1990s, with New Zealand followed by Australia being the highest of the four. While indigenous suicide in each of these four societies will be considered, for the reasons suggested above, particular attention will be given to Aboriginal suicide in Australia.
Patterns of Suicide Rates
Increasing rates of young male indigenous suicide in the United States have been documented from the 1950s, with rates varying across the nation from 8 to 120 per 100,000. Contemporary rates for young people are some three to four times higher than for the nation as a whole, with two-thirds of all indigenous suicides between the ages of fifteen and thirty-four being male. Violent means are the norm with firearms being responsible for over half of all indigenous suicides. A similar picture is found in Canada with a significant increase in suicide rates for indigenous young adult males in the 1970s. In 1987 the National Task Force on Suicide in Canada reported that suicides accounted for 15 to 20 percent of all violent deaths of native people in the early 1980s, with 60 percent of suicides occurring in those aged fifteen to twenty-four, at a male to female ratio of three to one. As in the United States violent means are common, but with a greater and increasing proportion of deaths as a result of hanging and with the proportion of deaths from firearms declining. As noted earlier, New Zealand as a nation has the highest suicide rate for young men of any of these four countries. Even so, Maori suicide rates were 50 percent higher for young men aged fifteen to nineteen years in the mid-1990s, with rates for males aged fifteen to twenty-four having peaked in 1989 at 49 per 100,000. Violent means, particularly hanging, are the norm and, as in Australia, attention has been brought to this issue as a result of deaths in custody.In Australia indigenous suicide has been recognized as a major issue only since the late 1980s, having been brought to public attention by the Royal Commission into Aboriginal Deaths in Custody. Although the excess of indigenous suicide deaths in custody eventually was found to be a result of the massive overrepresentation of Aboriginals among those in police and prison custody, the attention and coverage of hanging was intense and supported the development of public perceptions and understandings of Aboriginal hanging that included a political dimension. It was a series of suicides in the custody of the State of Queensland in the mid-1980s that led to the formation of the Royal Commission, and in that state suicide in the wider Aboriginal population subsequently increased some fourfold between 1992 and 1996. For the period 1990 to 1995 that state had a suicide rate of 14.5 per 100,000, with the Aboriginal and Torres Strait Islander rate being 23.6. The elevated rate is entirely accounted for by the increased indigenous male suicides among those aged fifteen to twenty-four (112.5 per 100,000) and those aged twenty-five to thirty-four (72.5 per 100,000), with these figures being 3.6 and 2.2 times, respectively, the rates for the state as a whole. Australian indigenous suicide is not only increasing and concentrated among young adult males, it is also unevenly distributed geographically and temporally with "waves" of suicides affecting particular populations at different times. This suggests a condition of community risk mediated by individual vulnerability to harm (including accidents, homicide, and other alcohol-related problems), of which suicide is but one manifestation.
Explanations for the Higher Suicide Rates
While explanations for suicide rates in indigenous populations are diverse and complex, all of the studies of this phenomenon emphasize the impact of the breakdown of cultural structures, processes, and integrity. Almost all such interpretations link these influences on culture to colonization and its consequences for social and family functioning as was summarized by the Canadian Royal Commission:Commissioners have concluded that high rates of suicide and self-injury among Aboriginal people are the result of a complex mix of social, cultural, economic and psychological dislocations that flow from the past to the present. The root causes of these dislocations lie in the history of colonial relations between Aboriginal peoples and the authorities and settlers who went on to establish "Canada," and in the distortion of Aboriginal lives that resulted from that history. (Royal Commission on Aboriginal Peoples 1995, p. 2)In Australia the historical context includes a period of enormous social change through the 1970s. Previously, indigenous lives and communities had been controlled through racist legislation, which began to lift only in the late 1960s. The next decade was characterized by political and social instability, the lifting of restricted access to alcohol, rapidly increasing rates of violence and accidents, high rates of incarceration, and many other manifestations of continuing turmoil and disadvantage, with serious consequences for the stability of family and community life. Aboriginal Australians who have taken their lives usually have been young men who grew to maturity during or since that period. They are members of the first generation to be exposed to the developmental consequences of widespread instability, much of which reflects the indirect effects of heavy alcohol use (particularly on paternal roles and, consequently, on male identity).
While such factors are critical to interpretation at a population level, they are mediated by effects on individuals. In a 1997 review of studies across these societies, Valerie Clarke, C. James Frankish, and Lawrence Green identified an association between suicide and factors relating to substance use and compromised mental health and self-esteem. The misuse of alcohol, particularly binge drinking, is a consistent association, as Anne Graham and her colleagues explained: "the script for 'drinking' in many indigenous communities includes binge drinking, anger over perceived past grievances and injustices, and suicidal ideation and injury" (Graham, et al. 2000, p. 13).
Most interpretations also highlight persistent social disadvantage. Studies in the early twenty-first century suggest, however, that the predisposition to suicide by vulnerable youth is influenced not only by absolute living standards but also by how they view their circumstances relative to those around them. Interpretations from Australia and Hawaii show that indigenous youth cite the widening gap between indigenous and Western cultures as an important factor in indigenous suicide.
A final consideration in explaining suicide rates in indigenous communities is that of "meaning." In indigenous settings, particularly in Aboriginal Australia, the occurrence of suicide and the circumstances of the indigenous communities mean that many people, including children, will have witnessed the aftermath of suicide. Clustering and the death by hanging of children, some as young as eleven years of age, in such communities suggests a powerful communicative and imitative dimension. At least in Australia, the communicative dimension of suicidal behavior has been influenced by events such as the Royal Commission into Aboriginal Deaths in Custody and by portrayals of hanging (as art, caricature, and graffiti) that associate hanging with political ends.
Intervention Programs
Intervention programs are necessarily informed by the service and policy frameworks in relation to suicide prevention and indigenous health across the four countries. These are significantly different. For instance, whereas there is a national Indian Health Service in the United States, in Australia indigenous health is largely the province of state health departments and, to a lesser extent, commonwealth-funded, community-controlled health services. Furthermore, initiatives related to indigenous suicide are encompassed within different national policy initiatives. For example, the Brighter Futures Program of Health Canada drives broad-based programs that address the social and cultural circumstances of young Native Canadians. In Australia there is as yet no nationally implemented indigenous health and well-being strategy, but partnerships with Aboriginal and Torres Strait Islander people form a key action area in the national framework for the prevention of suicide and self-harm.Such differences aside, there has generally been a transition in each nation from crisis-oriented interventions targeting at-risk individuals toward broader, multileveled strategic approaches. This was exemplified by the recommendations of the Canadian Royal Commission: "A comprehensive approach must include plans and programs at three levels of intervention: 1) those that focus on building direct suicide crisis services; 2) those that focus on promoting broadly preventive action through community development; and 3) those that focus on the long-term needs of Aboriginal people for self-determination, self-sufficiency, healing and reconciliation within Canada" (Royal Commission on Aboriginal Peoples 1995, p. 75). The commission reported that to be effective, programs should be community driven, holistic, and situated in a broad problem-solving approach. They should also balance crisis management with social agendas, place priority on children and youth, train Aboriginal caregivers, and encourage community-wide involvement.
In Australia suicide continues to increase in Aboriginal communities and is functionally inseparable from the wider picture of higher rates of disease, premature mortality, and social disadvantage. Perhaps because suicide has most recently emerged in Australia, the responses have remained ad hoc and largely crisis oriented although veiled by the ambiguous or evasive title of "life promotion" programs. There is, however, increasing recognition in policy and service planning of the need for a strategic balance of targeted and functionally accessible services and broad social interventions. For the indigenous peoples of each of these nations, empowerment and investment in the long term is needed to ensure the security of the environment of indigenous children.
See also: Causes of Death ; Suicide
Bibliography
Barber, James G. "Relative Misery and Youth Suicide." Australian and New Zealand Journal of Psychiatry 35 (2001):49–57.Baume, Pierre J. M., Chris Cantor, and Philippa McTaggart. Suicides in Queensland: A Comprehensive Study, 1990–1995. Brisbane: Australian Institute for Suicide Research and Prevention, 1997.
Clarke, Valerie A., James C. Frankish, and Lawrence W. Green. "Understanding Suicide among Indigenous Adolescents: A Review Using the PRECEDE Model." Injury Prevention 3 (1997):126–134.
Graham, Anne, Joseph Reser, Carl Scuderi, Stephen Zubrick, Meg Smith, and Bruce Turley. "Suicide: An Australian Psychological Discussion Paper." Australian Psychologist 35 (2000):1–28.
Hunter, Ernest, Joseph Reser, Mercy Baird, and Paul Reser. "An Analysis of Suicide in Indigenous Communities of North Queensland: The Historical, Cultural, and Symbolic Landscape." Report for the Commonwealth Department of Health and Aged Care, Canberra, Australia, 1999.
National Task Force on Suicide in Canada. Suicide in Canada. Ottawa: Mental Health Division, Health Services and Promotion Branch, Health and Welfare Canada, 1987.
Royal Commission on Aboriginal Peoples. Choosing Life: Special Report on Suicide among Aboriginal People. Ottawa: Royal Commission on Aboriginal Peoples, 1995.
Sakinofsky, Isaac, and Antoon Leenaars. "Suicide in Canada with Special Reference to the Difference between Canada and the United States." Suicide and Life-Threatening Behavior 27 (1997):112–126.
Shore, J. H., and S. Manson. "American Indian Psychiatric and Social Problems." Transcultural Psychiatry Research Review 20 (1983):159–180.
ERNEST HUNTER DESLEY HARVEY
MEDIA EFFECTS
Widespread coverage of a suicide in the media has long been thought to be capable of triggering copycat suicides in the mass public. In fact, more than forty scientific papers have been published on the impact of suicide stories in the media on suicide in the real world. However, there have been some inconsistencies in the findings of this research. Some studies find significant increases in suicide after a widely publicized suicide story, while other research finds no effect. The following entry reviews the research evidence with four goals in mind. First, what hard evidence is there for a copycat effect? Do suicidal people actually imitate suicides in the media? Second, how can this association be interpreted? What are the major theories that have been used? Third, what scientific generalizations can social scientists construct from the existing studies through a comprehensive analysis?Direct Evidence for a Media Impact
In 1774 the German poet Johann Wolfgang von Goethe's The Sorrows of Young Man Werther, a novel where the hero commits suicide due to a failed love affair, was banned in many European locations. It was perceived as responsible for imitative suicides in such places as Italy, Leipzig, and Copenhagen. Systematic scientific investigations on copycat suicide began with the work of the doctor David Phillips of the University of California in the 1970s. The largest possible copycat effect found was for Marilyn Monroe. During the month of her suicide in August 1962 there were an additional 303 suicides in the United States alone, an increase of 12 percent. In general, however, highly publicized stories increase the U.S. national suicide rate by only 2.51 percent in the month of media coverage.Most of the evidence for a copycat suicide effect is very indirect and usually weak. That is, associations are drawn between the presence of a suicide story and a rise in the social suicide rate. This rise is often demonstrated to be independent of other social conditions such as season, year, holidays, and the state of the economy. However, it typically is not known to what extent the people committing suicide are aware of the suicide story and if it had anything to do with their suicides.
Nevertheless, there is some convincing evidence for a direct copycat effect. For example, in the book Final Exit (1993), a guide to suicide for terminally ill persons, asphyxiation is the recommended means of suicide. In the year that Final Exit was published, suicides by asphyxiation in New York City rose by 313 percent from 8 to 33 suicides. Further, a copy of Final Exit was found at the scene of 27 percent of these suicides. Michel Tousignant and his colleagues studied seventy-one coroner's reports on suicides in Quebec in the month following a publicized suicide and found direct evidence of probable copycat effects. They determined that at least 14 percent of the suicides in the month following a widely publicized suicide of a popular Quebec journalist were at least partially linked to the story. For example, a number of the suicides were found with a copy of the suicide story nearby. In some cases the victim stated explicitly to significant others that he or she was going to imitate the suicide of the hero. Ninety percent of the suicides used the same method (hanging) as the role model in the story.
Explanations of Media Impacts on Suicide
Explanations of media impacts on suicide have generally been framed in terms of social learning theory. The simplest rendition is the imitation explanation, which argues that suicide stories are advertisements for suicide. Simply put, one learns that there are troubled people who solve their problems (e.g., divorce, terminal illness, dishonor) through suicide. Mentally troubled persons in society may simply copy the behavior of troubled people in the suicide stories. The content and presentation of suicide stories may be secondary to the basic message conveyed about problem solving. Research using this model generally lumps all varieties of stories together, making no distinctions among subtypes by celebrity status, age, gender, occupation, or other characteristics.A more complex set of explanations revolves around the learning process of differential identification. To the extent that people identify with a type of story, that type would be expected to have more of an impact. For example, men may be more apt to copycat the suicides of men than the suicides of women. If people tend to copycat the suicides of superior people, they would be expected to copy the ones of famous celebrities more than the suicides of ordinary people. Americans may identify more with the stories about American suicides than foreign suicides.
A third variety of explanation focuses not on story characteristics but on audience mood. Although this is the most understudied explanation for copycat suicide, the central thesis is that stories that appear when suicide-like conditions are high in society (e.g., high unemployment, high divorce, and low church attendance rates) have more of a copycat effect because more people are on the verge of suicide. Further, stories that appear in periods when suicidogenic conditions and moods are low will have less of an impact on copycat suicide.
Empirical Generalizations about Media Impacts on Suicidal Behavior
The researcher Steven Stack provides the only quantitative analysis of the findings of research studies to date. Stack's 2000 review is based on 293 findings contained in 42 scientific articles on the subject. There are essentially six solid generalizations that can be made about the conditions that maximize the relationship between the media coverage of suicide and suicidal behavior, including the characteristics of the suicide victim in the story (whether or not he or she is a celebrity), whether or not the suicide is real or fictional, the medium of coverage (newspapers or television), the dependent variable (suicide attempts or completions), the historical period of the analysis, and the amount of coverage of the suicide story. Two generalizations can be made on factors unrelated to the finding of a copycat effect: age range in the dependent variable and year of publication of the study.Celebrity suicides. Studies that measured the presence of stories regarding well-known entertainment and political celebrities were 14.3 times more likely to uncover a copycat effect than studies that did not do so. Researchers argue that suicide stories about such well-known people (e.g., celebrities, U.S. senators, and U.S. cabinet members) spark a greater degree of identification than stories about the suicides of other persons. The entertainment celebrity, in particular, has the greatest impact on copycat suicide. According to a reference group approach, if a celebrity figure with all her fame and fortune cannot endure life, the suicidal person may ask, "Why should I?" Along these same lines, a 2001 study of a well-known and respected journalist in Quebec has been associated with a substantial rise in suicide.
Real vs. fictional. Stack's analysis found that studies based on real suicide stories are 4.03 times more likely to report copycat effects than studies based on fictional suicides. For example, the several works on the four television movies about teenage suicide that aired in 1984 generally found no imitative effect. People may identify with true-to-life suicides rather than make-believe suicides in movies or daytime television dramas.
Medium of coverage. Unlike televised suicide stories, newspaper suicide stories can be saved, reread, displayed on one's wall or mirror, and studied. Television-based stories on suicide typically last less than twenty seconds and can be quickly forgotten or even unnoticed. Detailed studies of suicides occurring during media coverage of suicide have often found copies of suicide news stories near the body of the victim. Stack's analysis found that research based on televised stories was 82 percent less likely to report a copycat effect than research based on newspaper stories.
Dependent variables. While the models in suicide stories are almost always completers, Stack's analysis found that studies based on completed suicides as the dependent variables were 94 percent less likely to find a copycat effect than studies based on suicide attempts as the dependent variable. Possibly those persons most susceptible to copycat effects are those who are less determined to die.
Period effects. Research has been based on three principal historical periods: 1910–1920, 1929–1939, and 1948–1996. Research based on the 1930s is 93 percent less likely than 2001 research to find a copycat effect. This may be due to the lack of television to echo the stories covered in the radio and print media. However, it may also be due to the presence of massive social movements for social and economic change (e.g., labor movement) that may have distracted otherwise suicidal people from thoughts about suicide.
Amount of suicide coverage. Generally speaking, research has found that the greater the coverage of a suicide story the greater the chances of finding a copycat effect. Stack's analysis distinguished between studies based on one network's (e.g., ABC, CBS, NBC) coverage of suicides versus studies based on two or three network stories. The former were 84 percent less likely to find a copycat effect.
Age-specific suicide rates. Hypothetically, certain audiences (e.g., the very young and impressionable or the high-suicide-risk group of elderly white males) may respond more to publicized suicide stories than their counterparts. Stack's analysis distinguished between studies based on a dependent variable measuring youth suicide risk (ages 10 to 34), middle-aged suicide risk (ages 35 to 64), and elderly suicide risk (aged 65 and over). Studies based on young people were no more likely than studies based on the elderly to find a copycat effect. Further, studies based on middle-aged people were also not any more likely to find a copycat effect. However, nearly all studies in this vein did not match the age of the suicide victims in the stories with the age of the victims in the suicide rate being analyzed. Further work will be needed in order to systematically assess the impact of age identification on age-specific suicide rates.
Year of story publication. Sometimes as statistical techniques advance and standards for publication increase, relationships between an X and a Y variable may emerge or disappear. Stack's analysis found, however, that year of publication of a study was unrelated to the presence of a copycat effect.
Suicide Prevention: Media Guidelines
Professional organizations, including the American Association of Suicidology, have often prepared guidelines for the media to follow in presenting suicide story content. For example, they often advise the media not to mention the method of suicide and to avoid presenting photos of the suicide victim. It is not clear to what extent these guidelines were ever empirically validated. However, there is only one systematic study on this issue.One study that analyzes whether or not the guidelines are empirically validated was done by Phillips and his colleagues who studied characteristics of thirty-two televised suicide stories and their impact on teenage suicide in the United States. Twelve aspects of story content were measured, and included mention of the method of suicide, picture of the victim in normal life, picture of the victim's body or coffin, and whether or not the motive was specified. None of these characteristics of the stories was associated with significant increases or decreases in suicide risk. That is, for example, stories that mentioned the method of suicide were no more likely to be associated with increases in teenage suicide than ones that did not mention the method.
From the present review of empirical generalizations, social scientists believe that media guidelines should focus on the amount of coverage given to the story. The media might best control suicide by having fewer and shorter stories on the subject. Further, moving them to the inside pages of newspapers might also help reduce suicide risk. Because the suicides of celebrities are by far the most likely to trigger copycat effects, it has been suggested that perhaps the media should pay less attention to these "newsworthy" suicides. Researchers believe coverage in the print media should be reduced because it triggers more copy-cat suicides than the electronic media.
Finally, the mention of the negative consequences of suicide (e.g., pain and disfigurement) in suicide stories might reduce the imitative effect. These features of suicide are typically not included in suicide stories. One exception is the case of the late 1970s mass suicide at Jonestown where bloated and rotting bodies were shown in news stories and suicide declined. The Jonestown-triggered drop in suicide may not translate to suicide stories not dealing with cults; however, this one neglected aspect of the presentation of suicide stories may offset any copycat effect if it were enacted as part of a media policy.
See also: Children and Media Violence ; Suicide
Bibliography
Lester, David. Why People Kill Themselves, 4th edition. Springfield, OH: Charles Thomas, 2000.Maris, Ronald, Alan Berman, and Morton M. Silverman, eds. Comprehensive Textbook of Suicidology. New York: Guilford, 2000.
Phillips, David P., Lundie L. Carstensen, and Daniel Paight. "Effects of Mass Media News Stories on Suicide, with New Evidence on Story Content." In Cynthia Pfeiffer ed., Suicide among Youth: Perspectives on Risk and Prevention. Washington, DC: American Psychiatric Press, 1989.
Stack, Steven. "Media Impacts on Suicide: A Quantitative Review of 293 Findings." Social Science Quarterly 81 (2000):957–971.
STEVEN STACK
MENTAL ILLNESS
The term mental illness involves emotional suffering and/or with some degree of incapacity to perform a job or maintain fruitful social relationships. The illness most commonly associated with suicide is major depression, which is typically accompanied by chronic sadness, loss of energy, and an inability to tackle daily activities. Although none of these symptoms necessarily leads to suicide, most suicides experience one or more of them. Two other mental illnesses often associated with suicide are schizophrenia and manic depression or bipolar disorder, both of which can involve mental confusion and usually require hospitalization. Alcoholism and drug addiction, with their attendant loss of control over emotions and actions, are also associated with suicide. Personality disorders involving an inability to control anger and impulses have also been noted among suicidal patients.Clearly mental illness does not always lead to suicide or even to suicidal thoughts. Some 30 to 40 percent of Americans experience some form of mental health problem during their lives, but only 1.5 percent of Americans die by suicide each year. Thus, the overwhelming majority of people with mental health problems do not take their own lives. Even if such people are given to suicidal ideas, the likelihood of their acting on those ideas is remote.
The majority of persons who commit suicide have experienced serious difficulties with their parents during childhood. More than half have been rejected, abandoned, or physically or psychologically abused. These early adversities may make them more likely to mistrust other people and less able to face difficulties such as marital separation or financial distress.
If most mental health problems do not lead to suicide, most suicidal persons do suffer from mental health problems. Studies from the United States, Canada, India, Taiwan, and Finland show that 90 percent of suicides have had a psychiatric problem during the year before their death. At least one-third were seen by a psychiatrist, and a majority of them had more than one problem (e.g., combination of drug abuse and depression).
Mental Health Problems Commonly Associated with Suicide
Almost half of suicides suffer from severe depression, and some researchers claim that as many as 10 percent of those suffering from a depression will eventually die from suicide. Yet depression alone will not trigger a suicide. For instance, twice as many women as men suffer from depression, but, in the Western world, men are three to four times more likely to die from suicide. People who suffer from melancholy, irritability, and lack of appetite—all well-known signs of depression—are not necessarily high risks for suicide. Those who suffer from more severe forms of depression, involving insomnia, memory difficulties, and unkemptness—are at greater risk for suicide. Errki Isometsä and her colleagues in Finland have found that only 3 percent of those who committed suicide and were suffering from depression had received adequate treatment with antidepressant medication.The most salient indicator of suicide risk among depressives is the feeling of hopelessness. This feeling is not an essential element of depression, but it appears when friends and family members lose patience with the victim of depression. Having some form of family or community support is a key to preventing depression. Countries with a strong tradition of community support often have low rates of suicide even if they have experienced civil wars and generally high rates of depression.
Suicide results in 10 to 15 percent of the cases of those suffering from schizophrenia or manic depression. According to various studies, one quarter to one-half of persons with manic depression attempt suicide. One of the reasons why these patients are at such a high risk is because they often abuse drugs and alcohol to relieve the tensions resulting from their mental symptoms. The period of greatest risk is the five years following a hospital stay. Finally, those who are more depressive than manic are at a correspondingly greater risk of suicide.
Schizophrenics are more likely to commit suicide at a younger age, with only one-third taking place after age forty-five. Careful research does not support the widely held belief that persons with schizophrenia decide to kill themselves when they are feeling better, as a means of avoiding a relapse into their previous emotional agonies. On the other hand, four out of five commit suicide during periods of aggravated confusion and depression. It is also important to note that 40 percent of schizophrenic suicides were not taking their antipsychotic drugs as specified. Alcohol abuse is not common among schizophrenics, but they usually require less alcohol intake to experience inebriation. The most common feature of schizophrenic suicide is recent hospitalizations. Such hospital stays are typically repeated and brief and often coercive—many of them the result of previous suicide attempts.
Mental Illness and Stages of Life
Suicide increased among adolescents and young adults in Canada and many countries of Northern Europe in the latter part of the twentieth century. Many experts associate this increase with a rise in depression in this younger age group during the same period. Adolescents do indeed now suffer from depression as much as adults do (more, according to some studies), and half of adolescents who die by suicide suffer from depression. According to one study, adolescent depression may last for just a short period before the final act, leaving little time for intervention.For older people, physical ailments are an important variable in suicide rates, but their frequency of psychiatric problems is just slightly less than in younger age groups. A serious handicap or illness is also a source of depression because it threatens self-esteem. In contrast to younger age groups, older people who die by suicide are more likely to suffer only from depression and seldom have multiple mental health problems. This circumstance renders their depression easier to treat.
The Role of Mental Illness in Suicide
Even if suicide is closely linked to mental illness, it does not follow that a rise in the rate of mental illness will bring about an increase in suicide since, as we have seen, the majority of people with some form of mental illness do not take their own lives. Furthermore, some countries with a low rate of suicide have a high rate of mental illness.Can suicide, then, be attributed to new types of mental illness brought on by social change? For instance, psychiatrists have taken increasing note of the phenomenon known "borderline personality," a disease characterized by high impulsivity and a sense of emptiness, which now accounts for twenty percent of psychiatric inpatients. Drug abuse and social exclusion may contribute to the severity of this condition, which presents a correspondingly higher risk of suicide because of its association with impulsive behavior. For this very reason suicide can be highly unpredictable and thus difficult to prevent. With some impulsive persons, fewer than twenty-four hours elapse between a traumatic episode such as a separation and a suicide attempt. This trait of high impulsivity is not only an element of mental illness; it may result from experiences of abandonment and abuse suffered during childhood. In this regard, observations on social primates early maternal deprivation leads to self-injurious behavior later on in life. The chemistry of the brain is likely to have a role in the transmission of this reaction.
When impulsivity is a major symptom of mental illness, parents, especially single mothers, often have less success in intervening in the case. Increasingly permissive child-rearing methods seem to have aggravated this problem because many parents—not only those with mentally ill children— find it increasingly difficult to control and socialize children's aggressive behavior.
Society's attitudes of exclusion toward mentally ill persons can also make them more vulnerable to suicide. Once consigned to asylums, increasing numbers of the mentally ill now find themselves relegated to fending for themselves in the harsh milieu of metropolitan inner cities, perhaps interrupted by repeated short stays in hospitals in times of crisis. The health services other than hospitals are often insufficient to ensure that these patients have a decent quality of life. And among psychiatric patients, those who die by suicide tend to have been abandoned by their families.
Recent scholarship has identified a series of indicators for suicide risk in mental patients that have little to do with any specific psychiatric illness. The main characteristic is the state of hopelessness. The second is obsession with a single problem, a state referred to by suicidologists as "tunnel vision." The third indicator is social withdrawal, and the fourth is avoidance of activities.
Some genetic factors related to impulsivity have also been identified as a possible key to suicidal behavior, especially in cases of manic depression or bipolar disorder. But this genetic component cannot explain sudden changes in the rate of suicide in a population.
Finally, that the burden of psychiatric illness is aggravated by the onset of a physical illness in suicide. Some 40 percent of suicide victims suffer from a serious physical illness such as cancer or a neurological disorder.
Prevention and Intervention
Suggested preventive measures vary widely. An increase in antidepressant prescriptions in Sweden, Denmark, and Hungary has been accompanied by a decrease in suicide. However, during this period Scandinavian countries have also developed elaborate psychosocial suicide prevention programs. In contrast, in China, where the suicide rate is high, only 5 percent of those suffering from depression receive proper care. Antidepressant medication can become a factor in reducing suicide in the future, especially if accompanied by some form of psychotherapy and adequate social support.As of 2002, more programs have been developed by psychiatric teams to follow up patients after a hospitalization for a suicide attempt. A plan to provide those persons with a green card giving priority to crisis intervention services in case of emergency has produced positive results in England.
About one-third of people who commit suicide are under psychiatric care. Many of them are not easy to treat, and they do not always take prescribed medications as indicated. More than three-quarters do not manifest any suicidal intent to their doctor, making screening very difficult. Yet new treatment methods for some of the most difficult suicidal cases, self-centered and impulsive alcoholic men, are bringing some hope. For example, the program implemented by Anthony Bateman and Peter Fonagy in England requires an extensive professional investment in group and individual therapy lasting over a year and a half, but this is less costly than the medical treatment of repeated suicide attempts.
See also: Suicide ; Suicide Basics: Epidemiology ; Suicide Influences and Factors: Biology and Genetics, Culture
Bibliography
Bateman, Anthony, and Peter Fonagy. "Effectiveness of Partial Hospitalization in the Treatment of Borderline Personality Disorder: A Randomized Controlled Trial." American Journal of Psychiatry 156 (1999): 1563–1569.Brent, David A., et al. "Adolescent Psychiatric Inpatients' Risk of Suicide Attempt at 6-Month Follow-up." Journal of American Academy of Child and Adolescent Psychiatry 32 (1993):95–105.
Isometsä, Erkki T., et al. "Suicide in Major Depression." American Journal of Psychiatry 151 (1993):530–536.
Jamison, Kate Redfield. "Suicide and Bipolar Disorder." Journal of Clinical Psychiatry 61 (2000):47–51.
Roy, Alec. "Genetic and Biologic Risk Factors for Suicide in Depressive Disorders." Psychiatric Quarterly 64 (1993):345–358.
MICHEL TOUSIGNANT
PHYSICAL ILLNESS
According to a variety of studies suicide is more common among people suffering from physical illness. In addition, people with irreversible illnesses are much more likely to take their own lives than healthy individuals. Still, a minority of those who suffer from physical illnesses take their own lives, invariably well under 8 percent. Nevertheless, not all physical illnesses are related to increased suicide risk. Therefore it is important to understand why some individuals who are physically or terminally ill commit suicide while others do not.Common Physical Illnesses Related to Suicide
In 1986 the researcher Francis Whitlock summarized the results from fifteen published research studies of suicide which include information on physical illnesses and found that when psychiatric and geriatric patients are excluded about one-third of persons who died by suicide had a physical illness at the time of their death. The studies varied, reporting 25 to 70 percent of patients as having a physical illness. Furthermore, the physical illness could be conceived as an important contributory cause of the person's death in between 11 percent and 51 percent of the cases. Almost a decade earlier, the researchers Donna Myers and Charles Neal reported that psychiatrically ill persons who committed suicide were, in almost 30 percent of the cases, also physically ill. Illnesses that are related to increased suicide risk include epilepsy, cerebral disease, Huntington's chorea, Parkinson's disease, cancer, gastrointestinal disease, renal disease, and AIDS (acquired immunodeficiency syndrome).Epilepsy. A study conducted in England found that the risk of death by suicide among epileptics is 5.4 times greater than in the general population and about 5 percent of deaths by people suffering from epilepsy were suicides. The risk of suicide in females with epilepsy is twice that of males. There is little research indicating why those people suffering from epilepsy have a higher suicide risk.
Head injuries and cardiovascular disease. Major depression is associated with cerebral disease. Therefore, because of the significant link between depression and suicide, it is not surprising that there is a greater risk of suicide among persons who have sustained head injuries or who have had cardiovascular disease and also have symptoms of clinical depression. In a 1980 study conducted by Francis Whitlock and Mark Susskind, there was a six times greater prevalence of cardiovascular disease among suicide victims than the general population.
Huntington's chorea. When it was originally named in 1872 Huntington's chorea was described by George Huntington as a disease "with a tendency to insanity and suicide" (Adams 1994 p. 262). According to Whitlock, although about 7 percent of noninstitutionalized patients with Huntington's disease will eventually die by suicide, this is still a much greater proportion than in the general population. More than half of the suicides occur when individuals first showed signs of the early stages of the illness.
Parkinson's disease. In 1955 the researcher Peter Sainsbury found that the number of cases of Parkinson's disease among the suicides in England was 200 times greater than persons not suffering from Parkinson's disease. He interpreted the greater suicide risk as being associated to the higher rates of depression among Parkinson's sufferers.
Cancer. Studies indicate that there are fifteen to twenty times more people suffering from cancer who eventually commit suicide than those who do not suffer from cancer. Although one might expect that people with cancer would commit suicide fairly late in the development of the disease when they were more debilitated or experiencing more pain and suffering, studies show the opposite: The highest rate of suicide appears to be in the first year after the patient has received notification of the diagnosis. Most cancer patients are chronically depressed (80%), but so are suicide victims who are matched according to various epidemiological factors but do not have a cancer history (82%). In a 1995 review of studies indicating the prevalence of depression in cancer patients, the researcher Mary Lynch found that between 3.7 percent and 58 percent of cancer patients could be diagnosed as suffering from depression. However, only 5 percent of depressed cancer patients die by suicide.
Medical professionals know little about why some cancer patients who are depressed end their lives by suicide and others do not. Most researchers stop looking further once they determine that the person was depressed. When one considers the cause of depressive symptoms in cancer patients, one finds that depression is sometimes secondary to organic causes such as side effects of anti-cancer drugs and other pharmacological therapies. Depression may be a reaction to the crisis of having cancer or a reaction to pain and suffering that is not sufficiently controlled. In 1983 the researchers Letie Hansen and Charles McAler found that health care professionals were more likely to condone suicide in terminal cancer patients than in patients with other diagnoses. They found that the acceptance of suicide in their patients was more likely to occur if the practitioners had a high degree of death anxiety themselves.
Gastrointestinal disease. There are between two and one-half and eleven times higher rates of peptic ulcers among suicide victims than in the general population. Medical researchers interpret the high rate of peptic ulceration among suicide victims as being due to alcoholism, since gastritis and ulceration of the upper gastrointestinal tract are found in those people who have a history of alcoholism. Further, alcoholics have a high risk of suicide with or without gastrointestinal disorders.
Renal disease and hemodialysis patients. Depression is common among patients with end-stage renal disease and hemodialysis patients. There is an at least 100 times greater suicide risk among dialysis patients than nondialysis patients. These rates would be higher if those who stopped treatment or failed to follow the treatment program were included as suicides in these studies.
AIDS. In a 1999 review of all studies on AIDS and suicide published to date, Brian Mishara concluded that there is a high risk of premature death by suicide among AIDS patients. However, there appears to be an even greater risk among people who first learn they are HIV (human immunodeficiency virus) positive and do not have any symptoms. There are results from autopsy studies that suggest that persons who inaccurately thought they had AIDS have committed suicide.
Explanations of the increased suicide risk among AIDS patients have focused upon depression. However, alternative explanations include the possibility that those who become HIV positive are more often from groups with a high risk of suicide to begin with, including homosexual men and intravenous drug users. Other hypotheses have included the possibility that the symptoms and pain associated with AIDS are related to increased suicide risk, or that diminished meaning of life or coping abilities associated with AIDS are related to suicide risk. In a longitudinal investigation of persons with AIDS conducted from 1998 to 2001, Mishara found that although depression and several other factors were associated with greater suicidal contemplation, when all the factors were analyzed together, the only significant ones that remained were the ways people with AIDS cope with problems and meaning of life.
Other physical illnesses. Several physical illnesses that one might expect to be associated with greater suicide risk have not been proven to increase the risk of suicide. For example, people with multiple sclerosis appear to have a relatively low suicide risk. Persons suffering from senile dementia and Alzheimer's disease do not have an increased risk of suicide and in fact may have fewer suicides. In the case of senile dementia and Alzheimer's disease, the lower suicide risk may be related to an inability to complete a suicide in those who are disabled by the disease or, alternatively, it may be that persons with senile dementia are not necessarily suffering. It is not clear whether or not there is a higher prevalence of suicide among persons suffering from cardiovascular diseases or hypertension. There have been cases of suicides among people with cardiovascular disease and hypertension, and in these instances medical professionals have suggested that medications used for the treatment of hypertension and cardiac disease may induce depression in many cases and thus may increase the risk of suicide.
People with disabilities and chronic non-lifethreatening illnesses are frequently diagnosed as having clinical depression. Some researchers feel that their diagnosis is an error because many of the symptoms of these diseases are also used to classify a person as depressed. Despite the frequent diagnosis of depression, there is no research evidence to confirm the hypothesis that persons with physical disabilities or chronic non-life-threatening illnesses are more likely to attempt or complete suicides than healthy individuals. A possible exception to this is people who suffer from asthma for whom there are clinical descriptions of deaths by suicide related to anxiety associated with the condition's symptoms. However, hard data on the number of persons suffering from asthma who commit suicide are not available.
Possible Explanations for the Link between Suicide and Illness
How can researchers, medical professionals, and social scientists explain the increased risk of suicide among people with serious or chronic physical illnesses? Most studies focus on the presence of depression and consider depression as if it were a "cause" of the suicide. However, depression is present among all suicide victims—those who are physically ill as well as those who are in good health. Furthermore, only a very small percentage of people who are depressed commit suicide and only a small percentage of people who are physically ill and depressed end their lives by suicide. For most people it seems logical to be depressed when a person suffers from a serious illness such as cancer or a physical disability. However, the depression may be a side effect of the illness itself or of medications used to treat the person. In some cases patients may be depressed because of their physical environment; for example, patients in a hospital are more depressed than patients who are terminally ill and treated in a hospice environment or in their own homes.Researchers believe it would be worthwhile to identify depression among those who are physically ill and then identify the causes of the depression. Once the causes of the depression are determined, treatment would be indicated. In some instances treatment may include prescribing an antidepressant medication or changing or adjusting the dosage of medication the person is currently taking. In other instances counseling or psychotherapy can be helpful. However, professionals must not overlook the possibility that the quality of life in terms of daily experiences and interpersonal interactions may be related to the depression as well. Furthermore, side effects of the illness may be better treated or improved and this may have an important effect upon depressive reactions.
The second major explanation of increased suicide risk is that it is associated with direct consequences of the illness, usually pain and suffering. In the case of cancer, uncontrolled pain is related to suicidal behavior. There is a general consensus in the medical profession that if a physician administers adequate pain control a patient's desire to hasten death by suicide may significantly decrease. Despite the link between pain control and suicide in cancer patients, it is not obvious that there is a link with pain in other illnesses. For example, in people with AIDS pain and suffering do not appear to be related to suicidal intentions.
There has been little research completed on the relationship between suicide and how people cope with their illnesses. The few investigations that exist suggest that how people cope with their illnesses and the social support they receive may be important factors in determining whether or not those who are seriously, chronically, or terminally ill desire to continue living.
Conclusions
Physical illness is not invariably associated with greater suicide risk; however, many people with physical illnesses have a much higher risk of suicide than the general population. Many illnesses and physical disabilities may not be experienced as negatively as the general population believes. For example, in the case of people with physical handicaps and many chronic degenerative diseases, the time when there is a greater risk of suicide varies, depending upon the particular handicap or disease. In the case of AIDS and with some cancer victims, there appears to be a greater risk of killing oneself after learning about the diagnosis, rather than later when the illness results in serious symptoms and handicaps. The timing of the suicide suggests that it may not be the illness that results in increased suicide risk, but rather people's fears about the future and concerns about living with or dying from the illness. These fears may be alleviated or reduced by professional counseling and support from family and friends during the early stages when the person first learns of the diagnosis.It appears that patients participating in hospice and palliative care programs are less likely to end their lives prematurely by suicide. If this fact were confirmed, it would suggest that greater availability of such palliative care may have an important preventive effect. However, hospice programs and palliative care are often only available to persons identified as "terminally ill" who have discontinued all treatments to prolong life. Many seriously ill persons do not benefit from the advantages of palliative care programs because they fail to meet criteria for being "terminally ill" or they have chosen to continue treatments despite the advances of their illness. Wider availability of hospice care programs as well as good palliative care services for those who are not yet terminally ill or for those have chosen to continue treatment may have a significant effect in preventing suicide with people who are physically ill.
It does not appear that the jurisprudence legislation in the Netherlands since the mid-1980s legalizing euthanasia has resulted in either a decrease or an increase in suicide among persons who are physically ill. Based on clinical knowledge, the best ways to prevent suicide among people who are physically ill are to develop protocols for identifying the potential sources of depression and to develop more effective means of treating depression. Furthermore, educators must change physicians' attitudes regarding suicide, since research shows that physicians are more likely to feel that a suicide is "justified" when a person is seriously or terminally ill. These attitudes may hinder appropriate identification and treatment of clinical depression. Besides treating depression it is important, particularly among cancer patients, to ensure that there is adequate pain management and control. Furthermore, any activities that improve the quality of life, social supports, and the amount of communication with family that are possible to employ would most likely result in preventing suicide.
See also: Aids ; Communication with the Dying ; Good Death, The ; Pain and Pain Management ; Suicide ; Suicide Types: Physician-Assisted Suicide, Rational Suicide ; Symptoms and Symptom Management
Bibliography
Adams, John Hume, and David I. Graham. An Introduction to Neuropathology, 2nd edition. Edinburgh: Churchill Livingstone, 1994.Hansen, Letie C., and Charles A. McAleer. "Terminal Cancer and Suicide: The Health Care Professional's Dilemma." Omega: The Journal of Death and Dying 14, no. 3 (1983–1984):241–248.
Henriksson, Markus M., Erkki T. Isometsä, Päivi S. Hietanen, Hillevi M. Aro, and Jouko K. Lönnqvist. "Mental Disorders in Cancer Suicides." Journal of Affective Disorders 36 (1995):11–20.
Lynch, Mary E. "The Assessment and Prevalence of Affective Disorders in Advanced Cancer." Journal of Palliative Care 11, no. 1 (1996):10–18.
Matthews, Wendy S., and Gabor Barabas. "Suicide and Epilepsy: A Review of the Literature." Psychosomatics 22 (1981):515–524.
Mishara, Brian L. "Synthesis of Research and Evidence on Factors Affecting the Desire of Terminally Ill or Seriously Chronically Ill Persons to Hasten Death." Omega: The Journal of Death and Dying 39, no. 1 (1999):1–70.
Mishara, Brian L. "Suicide, Euthanasia and AIDS." Crisis 19, no. 2 (1998):87–96.
Myers, Donna H., and Charles D. Neal. "Suicide in Psychiatric Patients." British Journal of Psychiatry 133 (1978):38–44.
Sainsbury, Peter. Suicide in London: An Ecological Study. London: Chapman and Hall, 1955.
Whitlock, Francis A. "Suicide and Physical Illness." In Alec Roy ed., Suicide. Baltimore, MD: Williams & Wilkins, 1986.
Whitlock, Francis A., and Mark Susskind. "Depression As a Major Symptom of Multiple Sclerosis." Journal of
In one of several controversial lawsuits that blame rock music for a suicide death, Ozzy Osbourne, at a 1986 press conference in Los Angeles, denied all allegations that his song "Suicide Solution" was responsible for the death of a young boy who shot himself.
BETTMANN/CORBIS
BRIAN L. MISHARA
ROCK MUSIC
Suicide as a rock music trope can have many meanings, including rebellion against established social norms, sometimes to the point of nihilism; criticism of authority figures, such as teachers, politicians, and parents; and evocation of emotional traumas. Often these songs use sarcasm to register disenchantment with society, family, interpersonal relationships, or life itself. In much the same way that Jonathan Swift's "A Modest Proposal" suggests that the starving Irish should eat their plentiful children, many rock songs suggest suicide, whether intentionally or unintentionally, as a response to the listeners' troubles.Beginning in the 1980s, a series of wrongful death lawsuits focused public attention on the purported link between rock music and suicidal behavior. It seemed to many that rage-filled, overtly anti-establishment songs were actively encouraging adolescents to commit suicide. The rock group Judas Priest was alleged to use "subliminal" messages encouraging suicide. In the late 1990s concerns about the effects of music lyrics and controversial artists like Marilyn Manson resulted in a public hearing before the U.S. Senate. While no wrongful death suit has been prosecuted successfully against an artist and no empirical evidence exists that rock music in general, or any artist in particular, has directly caused any teen suicides, controversial music and musicians remain under scrutiny from scholars and officials who suspect a connection.
Although some may believe that only the most angry and nihilistic music includes suicidal themes, instead, it has been used by a wide variety of artists. Simon and Garfunkel, in their landmark 1966 album The Sounds of Silence, included two songs about suicide. One of them, "Richard Cory," is an adaptation of the well-known Edward Arlington Robinson poem that describes a community's shock when a rich and well-respected person commits suicide. Written in the turbulent 1960s, this song challenges the assumption that financial success is the measure of happiness. A very familiar song is "Suicide is Painless," the theme to the movie and television show M.A.S.H. While mainly known in its orchestral version, the lyrics describe the despair and hopelessness of suicidal depression. However, perhaps the most famous suicide song is decidedly non-mainstream Ozzy Osbourne's "Suicide Solution." The song lyrics, when taken out of context, can be interpreted as pro-suicide, but, in fact, the song as a whole is an ironic description of alcohol abuse as slow suicide: "Wine is fine, but whiskey's quicker / Suicide is slow with liquor."
Current research indicates that those most vulnerable to suicide often suffer from severe psychopathology, substance abuse, and/or extreme psychosocial stress. Hence, some analysts contend that music steeped in nihilism and social alienation may simply reinforce a suicidal predisposition stemming from other factors. Others point out that a vulnerable listener's extreme identification with a rock star whose behavior is suicidal or self-destructive can lead to imitation. A mitigating factor is the type of media coverage of celebrity deaths; since the 1994 suicide of Nirvana member Kurt Cobain, there have been confirmed reports of attempted or completed suicides by fans of his music and lifestyle, but not nearly the number feared. As long as there are rock stars whose music and lives romanticize the daring and rebellion of self-destructive behavior, their possible influence over the lives of their devoted followers will continue to raise questions and concerns.
See also: Suicide Influences and Factors: Media Effects ; Suicide over the Life Span: Adolescents and Youths
Bibliography
Brown, E. F., and W. R. Hendee. "Adolescents and Their Music: Insights Into the Health of Adolescents." Journal of the American Medical Association 262 (1989): 1659–1663.Gould, Madelyn S. "Suicide and the Media." Annals of the New York Academy of Sciences 932 (2001):200–224.
Jobes, D. A., A. L. Berman, P. W. O'Carroll, S. Eastgard, and S. Knickmeyer. "The Kurt Cobain Suicide Crisis: Perspectives from Research, Public Health, and the News Media." Suicide and Life-Threatening Behavior 26 (1996):260–269.
Litman, Robert E., and Norman L. Farberow. "Pop-Rock Music As Precipitating Cause in Youth Suicide." Journal of Forensic Sciences 39 (1994):494–499.
Phillips, D. P. "The Influence of Suggestion on Suicide: Substansive and Theoretical Implications of the Werther Effect." American Sociological Review 39 (1974):340–354.
Scheel, K. R., and J. S. Westefeld. "Heavy Metal Music and Adolescent Suicidality: An Empirical Investigation." Adolescence 34 (1999):253–273.
Stack, Steven. "Suicide: A 15-Year Review of the Sociological Literature. Part I: Cultural and Economic Factors." Suicide and Life-Threatening Behavior 30 (2000):145–162.
LAURA PROUD KEITH CHENG
Read more: http://www.deathreference.com/Sh-Sy/Suicide-Influences-and-Factors.html#ixzz2raIfzzD6

No comments:
Post a Comment